
Part of the Series
Despair and Disparity: The Uneven Burdens of COVID-19
Honest, paywall-free news is rare. Please support our boldly independent journalism with a donation of any size.
Early carnivals offered political power a safety valve. For a few days a year, rich and poor switched positions. The poor ran society (if in ritual only), except, when things were going badly in the everyday, the reversal suddenly turned into open rebellion from below.
In the present pandemic, it’s the powerful who are running a months-long masquerade, taking off masks ironically enough, in the face of all the evidence that the pandemic is marching on and mask mandates in combination with vaccines and other interventions can protect populations from infection.
The ruling class’s public health putsch aims to free a precarious just-in-time capitalism from supply chain gluts and social welfare obligations that a serious pandemic imposes. Better let people get sick or die than violate such a society’s prime directive placing profits first, the political class plots.
SARS-CoV-2, the COVID-19 virus, is cycling through new variants every two months, tinkering with both the human immune system and our already precarious vaccine coverage. The reduced deadliness the virus seems to represent at the moment, as some experts pronounce, isn’t a set outcome. It’s only one of multiple possibilities. As hospitalizations, which doubled under the BA.5 variant, underscore, sudden surges in virulence are also possible, perhaps even likely as the virus is being left to explore its evolutionary possibilities.
The virus, meanwhile, keeps knocking thousands into the Long COVID side pocket, where patients are lost to complex combinations of chronic conditions that medicine is finding difficult to treat.
The State of the Pandemic
Where are we in the global pandemic? The Johns Hopkins Coronavirus Resource Center reported another 7.16 million new COVID cases worldwide for the week ending July 31 (see the red time series on the right of the John Hopkins dashboard). That’s more new weekly cases than for any other COVID wave except Omicron this past winter.
The number of global weekly deaths underwent another increase to 16,400 deaths the week ending July 31, although representing fewer cases than in previous waves (the white time series on the right of the Johns Hopkins dashboard). Forty-two million new vaccinations were administered that week worldwide (the green time series).
The New York Times is mapping COVID hotspots in the Americas, Europe, Asia and Australasia. There in purple, France, Germany, Austria, Italy, Greece, Taiwan, Australia and New Zealand continue to be epicenters in average daily new cases per 100,000 population. In recent weeks, Costa Rica, Finland, Japan, South Korea, and Thailand all returned to hotspot status. Canada, Mexico, Brazil, Peru, Bolivia, Argentina, Tunisia, Armenia, Kazakhstan, Iran, Iraq and Mongolia hosted recent increases in caseloads. Panama, Botswana, Portugal, Spain and Norway saw declines from late June.
The seven-day average of daily confirmed COVID cases per million people from the beginning of the outbreak shows the present hotspots are trending in different directions. Taiwan and Italy’s outbreaks appear in decline. Greece and Finland are hosting large new spikes. Japan, South Korea, and Mongolia are hosting new surges. Australia, New Zealand, France, Italy and Germany continue to cycle through their months-long epidemics. The U.S., the U.K. and Brazil are reporting slow but steady increases. We see that none of the countries highlighted are reporting national testing data as of July 3 (click on “color by test positivity”).
For the COVID deaths per million people for these same countries, we see that the U.S., Brazil and Germany are showing slight increases. Italy, the U.K. and Australia are showing more robust increases, and Costa Rica, Finland and Greece are displaying sharp spikes.
The virus also continues to evolve. This is a family tree for COVID samples over the past six months, although, for the radial version of the tree, rooted from the beginning of the pandemic at the center of the diagram and branching outward as SARS-2 evolves. We see in dark blues and purples the early variants like Alpha and Beta. In the light blue are samples of the Delta variant. We see over the past six months that multiple Omicron subvariants — there in yellow BA.1 and 2, in the light and medium oranges BA.4 and 5, and the darker orange BA.2.12 — are continuing to explore SARS-2’s evolutionary space. Indeed, we see in the few red samples the arrival of subvariant BA.2.75 or the Centaurus variant found first in India in June.
Across the Omicron group, we find molecular changes from the root of the SARS-2 tree here numbering as high as 64 amino acid changes and 16 deletions. What that means is that the virus continues to evolve, along the way experimenting with the human immune system to the tune of over 7 million new infections a week during what governments worldwide are treating as the end of the pandemic.
Hospitalizations are all up in the countries in our highlighted set. These appear as a function of the surge in caseloads, the reemergence of deadlier subvariants such as BA.5, and a developing mismatch between Omicron and COVID vaccines. We also see across countries in our set a near-global retraction in nonpharmaceutical interventions since Omicron. These indices of the stringency of public health measures show that some countries at first attempted to differentiate masking mandates and the like for the vaccinated (in green) and for the unvaccinated (in brown) before largely abandoning that distinction.
That combo — evolving subvariants probing our defenses and a willful public health surrender — bodes ill for this winter’s likely surge.
The U.S. Outbreak
As of August 7, the U.S. continues to host a raised floor in COVID-19 caseloads post-winter Omicron. This summer marks the worst in U.S. COVID-19 incidence of the three summers so far in this pandemic.
The New York Times map shows Northeast and upper Midwest are presently characterized by a relative decline in COVID. But we also see the start of a possible new surge in New Jersey, New York City and now, Pennsylvania. We see sharp spikes in Appalachia, particularly in Kentucky and West Virginia. The South is hosting lifted floors, especially in North Carolina, northern Louisiana, the Florida panhandle, Miami, parts of Alabama and Georgia, Oklahoma overall, and select counties in west and south Texas. We see a slight decline along the West Coast, a steady surge in parts of the Southwest, and sharp spikes county-by-county across the Plains states. Alaska and Puerto Rico continue to be hit badly.
There are other ways of tracking COVID. The levels of SARS-2 virus detected in the wastewater that comes through our sewage plants as reported here (July 19-August 2) shows little change from earlier in July. Sewage plants in red represent loads at 80 to 100 percent their previously recorded levels. We see these scattered across the U.S., but especially in Nebraska, Illinois, Ohio, Kentucky, South Carolina and downstate New York. The cool blues of recorded lows in the Northeast are starting to be infiltrated by increased SARS-2 concentrations in orange from New Jersey up north. We do see cooling off in coastal Washington State, Oregon and northern California.
The map of percent change in the last 15 days underscores the West Coast’s cooling off. We see such declines in light blue of 10 to 90 percent across Utah, Colorado, Nebraska, and what we were worried about in the first wastewater map in downstate New York. These might represent only mean declines off very large peaks that still host widespread COVID. At the same time, we see new 15-day surges in Illinois, Ohio, upstate New York, Kentucky and North Carolina.
A standing problem in tracking COVID-19 stateside is that the U.S. appears to be willfully ignoring previous surveillance measures. In April, ABC News and other outlets reported that the Department of Health and Human Services ended the requirement that hospitals report daily COVID deaths, overflow and ventilated COVID patients, and critical staffing shortages. Some U.S. states outright ended reporting COVID metrics, hospital bed usage and availability, and ventilator use. Some states turned to delaying COVID-19 numbers to reports on a weekly basis.
The ABC News report continued that some hospitals are following the National Institute of Health’s lead in changing definitions of COVID cases, including to only those patients that receive antivirals remdesivir or dexamethasone. So COVID cases wouldn’t be counted unless the patient needed those drugs.
It appears the willful decline in monitoring is beginning to extract its public health costs. For instance, we see here in San Francisco that previously SARS-2 loads in sewage (in blue) tracked COVID caseloads (in red). That appears no longer to be the case, with COVID caseloads during BA.4 and 5 likely to be underreported.
To sum up U.S. COVID, we see almost the entire country — 94 percent of U.S. counties — under “Data Type: Community Transmission” in the CDC maps is filled in at the highest level of community transmission, including what were a month ago sites of COVID decline in Iowa, Pennsylvania and New York State. The summer surge is accumulating with much of the country still reporting in COVID-19 tests at 20 percent or more positive (click on “Nucleic Acid Amplification Tests (NAATs)”). And much of the country — especially through the South, Appalachia and the Plains states — with less than 30 percent of the population with two COVID vaccine shots, even before including subsequent boosters (click on “Vaccinations” on the left and “% of total population fully vaccinated” on the right).
Monkeypox Marks Another Roll of the Epidemiological Dice
As on the global stage, SARS-2 continues to evolve here in the U.S. We see here new variants first emerging and then dominating in cycles of every two months. The BA.2 Omicron subvariant in pink was replaced by the BA2.12 subvariant in orange, which is now being replaced by subvariants BA.4 and 5 in green, with BA.5 surging ahead to account for over 85 percent of new cases as of July 30.
Each new COVID variant marks the U.S.’s — and the world’s — concerted failure to control infectious disease. Entirely new pathogens underscore the point. Monkeypox — a previously marginal Orthopoxvirus that can induce at times very painful lesions in the anus, genitals and mouth — has spread to all but two U.S. states, with patients getting little access to follow-up care or the vaccines that at best offer disease mitigation.
Epidemiologist Kathryn Jacobsen reports that the federal government’s recent declaration that monkeypox represented a U.S. public health emergency opens up more of such resources. The declaration, while welcome, is a month too late from helping quash an outbreak once limited to a few urban epicenters. The declaration also serves more as a guideline for local public health departments as to reporting and treatment, but not how to intervene or to help the greater community respond, with schools about to reopen at the end of August.
That is, the failures of the COVID response stateside have been set on repeat. The damage isn’t merely a matter of the surprise of a new outbreak or which political party is in power. The fiasco is systemic and extends back into the disease cascade.
Each new emergent pathogen represents a roll of the socioecological dice. Deforestation and development in the far reaches of capitalist production are springing even the most marginal pathogens out onto global trade and travel networks to reach countries that have taken great pride in destroying their own public health systems in the name of open economies.
Here, Rebecca Levine’s team maps its ecological niche model of monkeypox distribution across Sub-Saharan Africa, including in a Congo Basin that since has suffered considerable deforestation, especially there in the purple.
While most land deals underlying extraction in the Congo Basin are European and Asian in origin, the Land Matrix Observatory identified seven deals with direct American investment, including a 348,000-hectare deal with U.S.-registered Congo Emissions Management and Groupe Blattner Elwyn. Although this latter deal appears to be pursued under the rubric of carbon offsets, such agreements in green capitalism score their damage in helping rationalize offshore capital’s right to the Global South.
Many of the European and Asian efforts in the Congo and across West Africa meanwhile end up supplying U.S. customers, including wood siding to retailers Home Depot and Menards.
The defacement only compounds in its effects. When the Global North refused to follow through with a promised $500 million to the Democratic Republic of the Congo (DRC) to preserve its rainforest, the DRC, looking to Angola and Nigeria’s path of development, turned to auctioning off its forest to oil companies, including Virunga National Park, the critical gorilla sanctuary.
Monkeypox in the U.S. may be a matter of blowback. It’s not that any one of these land deals let loose this strain of the virus, but that pathogens are in part sprung when this model of development turns food forests into cleared land and expropriated resources marked by a loss in the environmental complexity that once bottled in those pathogens.
Two Additional Dangers
The capital-led destruction is also found on this side of disease spillover. Two additional dangers other than acute infections and deaths — the latter now projected at 17.5 million or more — arise from letting SARS-2 run free.
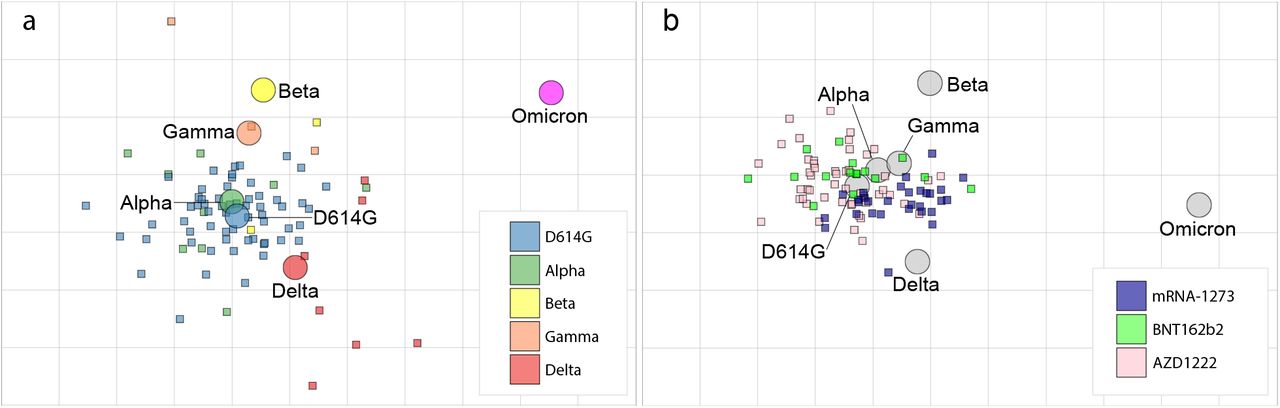
The first is that the virus may experiment enough to figure out how to emerge from our vaccines’ disease immunity — the protection the vaccines offer us from getting too sick when we’re infected.
One Dutch team of microbiologists produced what’s called an antigenic map to track vaccine coverage. The map on the left shows that the Omicron subvariant BA.1 evolved out from underneath the protection provided by being infected with earlier variants like Alpha, Beta and Delta. The map on the right tracks the antibody neutralization the vaccines provide in comparison to the circulating COVID variants. That map shows Omicron (in pink) has escaped the antibodies produced by the vaccines we’ve used to this point.
{kind=link}
That doesn’t mean the vaccines are useless, just that they don’t necessarily produce all the Omicron-specific antibodies.
Moderna is reporting its Omicron-specific vaccine in development to be successful. But we are likely in for boosters for years, with no guarantee a SARS-2 on a two-month schedule won’t continue to evolve out from underneath that protection.
The second danger is the Long COVID any one infection may induce or, perhaps, the cumulative impact of multiple COVID infections. A Weill Cornell Medicine team recently summarized the damage: On the left, the little graphs in red show the hazard ratios of all the body systems that have been documented to be impacted.
{kind=link}
The “Long” in Long COVID isn’t just the length of time of such an infection, but also represents a foundational transition from an acute respiratory infection to a chronic condition of often devastating impact. We’re talking about various combinations of cognitive impairments, ulcers, pulmonary fibrosis, embolisms, diabetes, fatigue, and many more illnesses in the list to the left of the human figure shown.
To the right of the figure, we see all the different drugs Long COVID patients are found to be at a higher risk of having to take.
That’s why the People’s CDC — the coalition of public health practitioners and everyday people I’ve joined — is adamant that all efforts must be made to implement a full array of public health interventions that keep all people, whatever their starting health, from entering the horror of Long COVID.
Biden’s Mask Off Shows Us Another Trump
In contrast, a Biden administration elected to volte-face Trump on COVID turned its position 360 degrees back to Trump positions. In the face of an adaptive and ongoing pandemic that is producing nearly 7 million new infections a week worldwide and Omicron subvariants evolving out from under vaccine coverage, the Biden administration decided to declare victory on COVID-19.
NBC News reported that in February, Impact Research, the administration’s polling firm, recommended moving beyond merely dropping mask mandates and by default toward discouraging mask use.
Molly Murphy and Brian Stryker of Impact suggested that the administration make a play for November’s midterm elections and “declare the crisis phase of COVID over and push for feeling and acting more normal.” In what seem to be talking points from the problematic “Urgency of Normal” campaign that encouraged moving students back into schools without adjunct interventions, Murphy and Stryker cited learning loss at school and COVID’s effect on the economy as reasons to exit COVID as a reality.
Both problems arose out of decisions the Trump and Biden administrations made in refusing to provide adequate support for communities and households alike during a national crisis. At the same time, the Impact memo continued, aiming to eliminate COVID isn’t the answer. In effect, with language reminiscent of Trump’s Chief of Staff Mark Meadows, the memo admits that COVID will remain the reality, which Murphy and Stryker also suggest the Biden administration ignore.
The CDC, other administration officials, and outside epidemiologists would follow up the memo by warning the American people of upcoming COVID spikes, including this fall and winter when Americans go to the polls.
Such realities are socially structured. In early July, Anna Peele interviewed the soon-to-retire Anthony Fauci for the Washington Post magazine, under the headline, “The Pandemic Is Waning”:
I am also aware that it would be a moral crime to transmit the coronavirus to Fauci. So when I got COVID two weeks before our interview, I obsessively parsed the guidelines from the Centers for Disease Control and Prevention: As long as I waited 10 days after my first positive test, I could still meet Fauci in person, right? No, I was informed by Fauci, via a member of his communications team. I would need to test negative three days in a row and wear a mask, even outdoors.
So, no five-day quarantine for Fauci’s circle along the lines a CDC under employer pressure recommended for Americans. And Fauci treats the possibility of infection after 10 days as real. These are exactly the kinds of precautions the People’s CDC recommended for the rest of the country.
When Biden finally contracted COVID, showing up to work maskless while infected, CDC Director Rochelle Walensky took to the airwaves saying that, yes, the president would be treated with precautions above and beyond what the CDC recommended for the American people. After all, the Americans whom the administration abandoned make up the labor force that chooses to go to work sick or alongside sick coworkers. The CDC is only accommodating them:
Yeah, I think we can all agree that the president’s protocols likely go above and beyond and have the resources to go above and beyond what every American is able and has the capacity to do.
As we put forward our CDC guidance, we have to do so so that they are relevant, feasible, followable by Americans, and that is Americans that live in urban jurisdictions and rural jurisdictions, that have resources and less resources, that have, you know, work constraints and many other things. So, when we put forward our guidance, we do so so that they reflect such that every American is able to follow them.
A growing class divide, which mainstream public health must accommodate first and foremost in the folksiest of fatalism, is treated as more sacrosanct than the obligations to control and prevent an infectious pandemic.
The resulting damage is unlikely of any American’s choosing. “For the period from June 29 to July 11 [2022],” the Wall Street Journal reported, “3.9 million Americans said they didn’t work because they were sick with Covid-19 or were caring for someone with it, according to Census Bureau data. In the comparable period last year, 1.8 million people missed work for those reasons.”
Even steps forward act to fill in such continuing damage. The administration recently announced it would be establishing a new Department of Health and Human Services office dedicated to addressing the debilitating Long COVID that an estimated 23 million Americans are suffering beyond their initial acute infections. An associated National Research Action Plan on Long COVID is to be pursued alongside the administration’s efforts to “return to normal” and strip out programs in COVID prevention.
In other words, the supply of extremely difficult-to-treat Long COVID cases the administration now says it seeks to mitigate will continue apace to accommodate employers.
When Pandemic Play Turns Serious
Given the bipartisan push to end COVID as an idea (if not as an empirical fact), science writer Ed Yong’s sense of defeat may be more an acknowledgement that a different public health is possible. And that it’s already underway, with a passing reference to the People’s CDC:
In 2018, while reporting on pandemic preparedness in the Democratic Republic of Congo, I heard many people joking about the fictional 15th article of the country’s constitution: Débrouillez-vous, or ‘Figure it out yourself.’ It was a droll and weary acknowledgment that the government won’t save you, and you must make do with the resources you’ve got. The United States is now firmly in the débrouillez-vous era of the COVID-19 pandemic…
I have interviewed dozens of other local officials, community organizers, and grassroots groups who are also swimming furiously against the tide of governmental apathy to push some pandemic response forward, even if incrementally. This is an endeavor that all of American society would benefit from; it is currently concentrated among a network of exhausted individuals who are trying to figure out this pandemic, while living up to public health’s central tenet: Protect the health of all people, and the most vulnerable especially. The late Paul Farmer, who devoted his life to providing health care to the world’s poorest people, understood that when doing such work, victories would be hard-won, if ever won at all. Referencing a line from The Lord of the Rings, he once said, ‘I have fought the long defeat.’ In the third year of the COVID pandemic, that fight will determine how America fares against the variants and viruses still to come.
What Yong misses in his respectable summary is that the resulting patchwork isn’t just a reminder of what we have lost or what we might gain upon a reformation of a pivot, but perhaps a new world born out of the husk of the old.
With death and illness accumulating from one COVID variant to the next, and now with novel pathogen species like monkeypox joining the party, the ritualized protest that the capitalist carnival allows may suddenly lurch into open rebellion. Millions may organize to burn down that Venn diagram of going to work in an apocalypse. There is another option: they can refuse to get sick and die for profit’s sake.
An important fundraising appeal: 8 Days to raise $46,000
Thank you for reading Truthout today. We have a brief message before you go.
Unfortunately, donations are down for Truthout at a time when media faces immense pressure. Yet, grassroots media is vital in the fight against Trump’s authoritarian reign. Our mandate to tell the truth, share strategies for resistance, and speak against fascism grows more urgent each day. We must appeal for your support.
If you can support Truthout with a one-time or monthly donation, you will make a significant impact on our work. Please donate during our fundraiser.