Truthout is an indispensable resource for activists, movement leaders and workers everywhere. Please make this work possible with a quick donation.
As Secretary of Health and Human Services Robert F. Kennedy Jr. and his “Make America Healthy Again” (MAHA) acolytes readily admit, U.S. public health continues to deteriorate. Five years into the COVID-19 pandemic, U.S. life expectancy is at best stalled while those of other industrial countries have rebounded back onto their historical trends upward.
The solution Trump administration officials are offering is to replace 125 years of — albeit underfunded — public health infrastructure with a eugenics-framed program wrapped in natural health packaging.
During his swearing-in as the new director for the Centers for Medicare and Medicaid Services, Mehmet Oz presented this program in the terms of wartime sacrifice:
Like Health and Human Services Secretary Robert F. Kennedy Jr., Oz signaled his plans to focus on chronic disease in the U.S., saying it was “the patriotic duty of all Americans to take care of themselves.”
“Because it’s important for serving in the military, but it’s also important because healthy people don’t consume health care resources,” he added. “The best way to reduce drug spending is to use less drugs, because you don’t need them, because you’re healthy, and it feels a lot better.”
The message: Take care of yourselves — because we won’t.
Never mind the trillions of dollars Americans pay into a largely privatized — and very profitable — health care system, far outspending other industrial countries only to suffer worse health outcomes.
The new Trump administration is now compounding this long-standing damage by dismantling the last of the public commons.
It’s cutting billions to state programs tracking disease, repealing emissions and drinking water regulations, revoking hundreds of millions in funding for life-saving research, canceling local food programs for schools and food banks, rolling back vaccinations, and shutting down the Centers for Disease Control and Prevention’s (CDC’s) Healthcare Infection Control Practices Advisory Committee.
The administration is also truncating the bird flu response and Meals on Wheels; firing CDC’s sexually transmitted infections lab team; cutting the Occupational Safety and Health Administration (OSHA); dismembering the National Institute for Occupational Safety and Health; and reducing the Medicare programs Oz will supervise, as Congress weighs deep cuts to Medicaid, pricing the poorest out of health care to the public health cost of us all.
In these programs’ stead, MAHA aims to place responsibility for health problems on the individual. Americans must somehow eat better and sleep more while also working more hours than their European counterparts, for stagnating pay. Americans must now “do their own research” on complex medical matters beyond the due diligence that can reasonably be expected of any adult — as if each of us can serve as our own CDC.
Nothing inspires patriotism like blaming Americans for the societal damage the political class pursues in their name.
A Continuity We Must Cop To
Democratic Party politicos, largely state officials outside Washington, D.C., have objected to these rollbacks both in the press and in the courts. Many a Democratic accusation, however, also carries the ring of a confession.
Where, after all, did the Trump administration get the idea the pandemic was over and that it could strip out federal COVID-19 programs? Or that public health was a matter of “you do you” individualism? Wasn’t it only three years ago that President Biden’s CDC Director Rochelle Walensky took a eugenics position on the pandemic, claiming it was good news that it was largely people with underlying health conditions who were dying from COVID?
Who botched the latest bird flu response to begin with? What administration did nearly nothing around the toxic derailment in East Palestine, Ohio? Who green-lighted over a year of Palestinian genocide, with, we recently learned, even Israeli officials surprised President Joe Biden never pressed for a ceasefire and with Secretary of State Antony Blinken approving bombing Gaza aid convoys?
There’s a shared path across administrations leading to this public health moment — with whole populations at home and abroad increasingly abandoned. Any opposition movement must understand that these patterns began long before Donald Trump if it aims to fight back effectively.
The problem here is a structural crisis of capitalism and requires more than an electoral solution. The public commons no longer holds space within existing relations of private property and production. The bases of our shared society are being treated as disposable baggage, threatening the country’s very existence.
Why Public Health Must Be Collective
Under whichever political party, public health, by definition, can never be conducted as an individualist enterprise.
Yes, each of us has choices to make and responsibilities to attend to during a pandemic or other emergency, but — as the CDC missed even before Trump — effective public health isn’t merely an emergent property of many millions of individual choices. Public health requires collective decision-making. It requires action at scale — from the neighborhood level to global cooperation.
Our health is connected to people halfway across town or halfway across the world. Making sure we can mutually protect ourselves requires us to arrive at decisions together. Our society relies on this collective decision-making to protect our shared social health.
Modern employers — from the classical liberal era to neoliberalism and the now-accelerating turn toward a fascistic reorganization of government — have consistently opposed such an objective.
While some employers want the state to help keep the workforce healthy enough to be efficiently exploited on the job, other employers — and sometimes the very same ones — are perfectly willing to serve workers into the maw of occupational dangers in order to reduce expenses.
Elsewhere, employers and their proxies demand that funding for social services be redirected to industrial subsidies or tax cuts for the rich. Sick or dead employees can just be replaced from the reserve army of labor — the unemployed surviving on society’s margins — or, increasingly, by AI.
Countries differ in how they approach public health programming. National programs differed in their response to COVID and bird flu. But any such program must operate at scales of organization that match the scales of the problems jurisdictions face.
So no corporation, individual, or market can defeat a pandemic. Public goods like public health and clean water require other orders of intervention. We cannot shop our way out of problems in population health, which represent far more than the mere “externalities” corporations park off their balance sheets or the influencer marketing MAHA is attempting to turn into policy.
Public Health Is More Than a Good Idea
The connections between the structure of a society and its public health practices speak directly to bedrock notions of social justice and fairness.
Our collective health arises from the daily ergonomics of the workplace and the kinds of collective decisions we make around how to organize and run our neighborhoods and rural communities.
The notion that workers and residents could govern themselves from the bottom-up seems to many commentators beyond our increasingly top-down society. History, however, is replete with examples. For instance, Maroon communities were self-governing safe havens for self-liberated formerly enslaved people, often joining with Indigenous people throughout the southern hemisphere.
Historian Mike Davis describes the origins of Chambers of Commerce as a desperate employer effort to counter Chambers of Labor, another example, which fought for worker well-being from the factory floor to the neighborhood block.
With only Chambers of Commerce left today, the top-down version is now presented and operationalized as the natural order of things. In our hyper-individualist culture, the boss/employer/owners — and Kennedy, Oz, Walensky, and other officials in recent governance — aim to shift all responsibility for health outcomes, and all the blame, onto atomized individuals.
We see similar efforts in other sectors. The framing the oil industry attempted in making everything environmental a consumer choice also underlies the COVID-19 response. We cannot consume our way out of a pandemic, however, even with the best respirators or hand sanitizers on the market.
The labor movement structurally disrupts the notion that each of us alone is enough during a widespread health crisis. Most union members working on workplace safety instantly recognize and dismiss this “blame the worker” (and the worker alone) approach.
We could all benefit from learning to assimilate that recognition as a social gut instinct. The health of the country would likely improve if the public moved away from viewing its interests and well-being in the funhouse mirror of the employers and the political candidates that the wealthiest fund.
The Holes in Swiss Cheese Modeling
Such a pivot would also suit U.S. public health practitioners. Many public health models accept — and operationalize — the political premises of the institutions funding them, with significant impacts on our health interventions.
A variety of public health models, for instance, show only things that a worker or consumer can do during a crisis.
A common representation of this approach comes out of Ian Mackay’s adaptation of James Reason’s “Swiss Cheese” model for respiratory defense. Each “slice” of an intervention has its uses and problems. Layering the different kinds of interventions covers each slice’s functional holes. What masking misses, handwashing, eye protection and social distancing can likely catch.
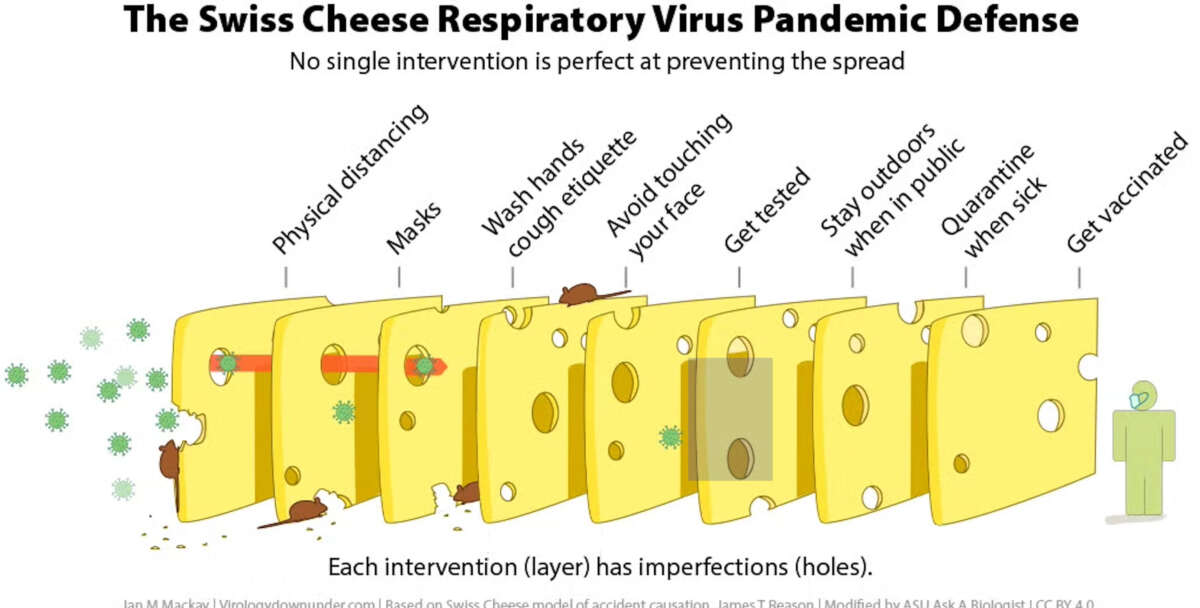
We see in such models always the “me,” never the “we.” Every intervention is the individual’s personal responsibility.
Hospital epidemiologist Saskia Popescu presents a broader version, showing what individuals can do — wear masks, get vaccinated — and what “we” can do collectively:
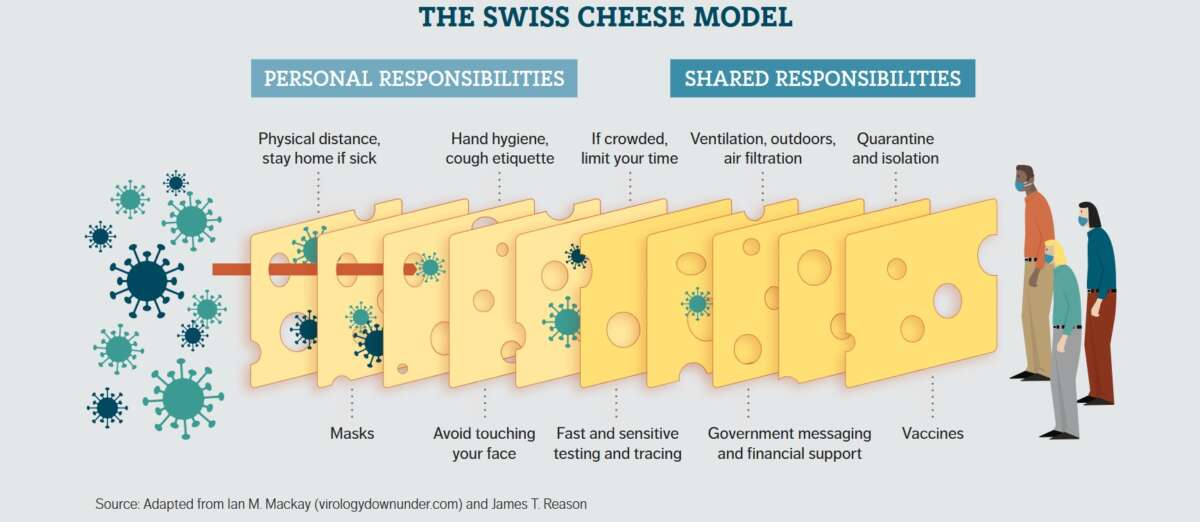
Yet “shared responsibilities” universalizes updating the HVAC system at your work, the downtown library or the neighborhood bar to no one in particular.
If everyone is responsible, then no one is responsible, and nothing is changed. “We,” “our,” and “shared” must always be explicitly identified. It’s the boss’s responsibility to provide clean air and personal protective equipment (PPE) at work, though perhaps the model is technically right in that without unions demanding clean air through bargaining or legislation, the intervention might not ever take place.
The abrupt end to federal pandemic protections guaranteed companies would stop providing paid COVID sick leave and other precautions (now including vaccination) on their own. Employers, as most people who call in sick know, hate paying people not to work.
Some employers chose a different path, if only in passing fashion. The University of Southern California (USC) adapted the Swiss cheese model to illustrate its own responsibility alongside the responsibility of individuals within that institution:
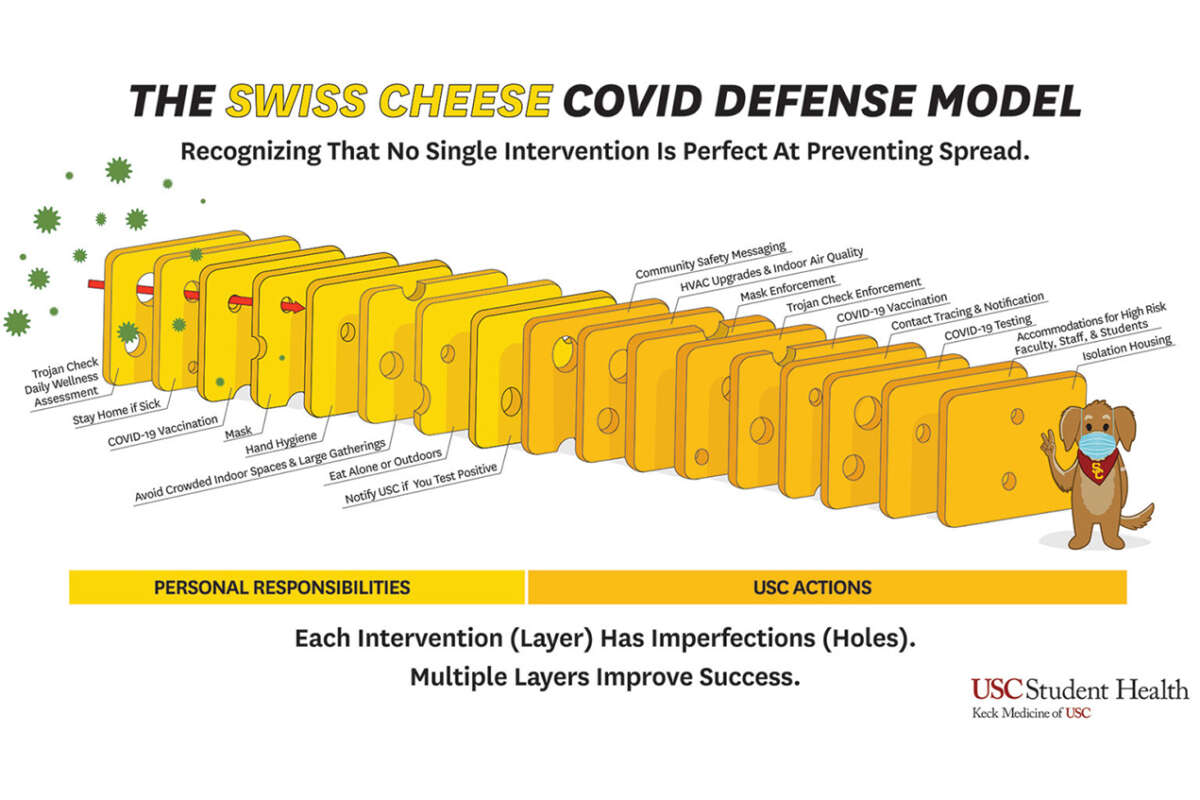
USC didn’t distribute free masks, but did provide testing, tracing and HVAC upgrades to good epidemiological effect.
Which health model institutions use shapes what they see as the nature of the emergency and what they choose to do about it. The model of personal responsibility isn’t entirely wrong — but it is woefully incomplete.
The most frightening model — the social Darwinism that encourages sacrificing elders or youth to the needs of the market — often went unspoken during the early pandemic (except for a shameless lieutenant governor of Texas here and there). As Oz’s press conference demonstrated, the soft eugenics of early COVID is now being increasingly deployed in more explicit language.
The Swiss cheese model provides an excellent, accessible tool for grasping multilayered problems and their solutions. We now need to keep track when modelers and policy makers leave out whole blocks of slices that make the critical epidemiological difference. We cannot let the growing holes in the model be normalized.
Hierarchy of Public Health Control
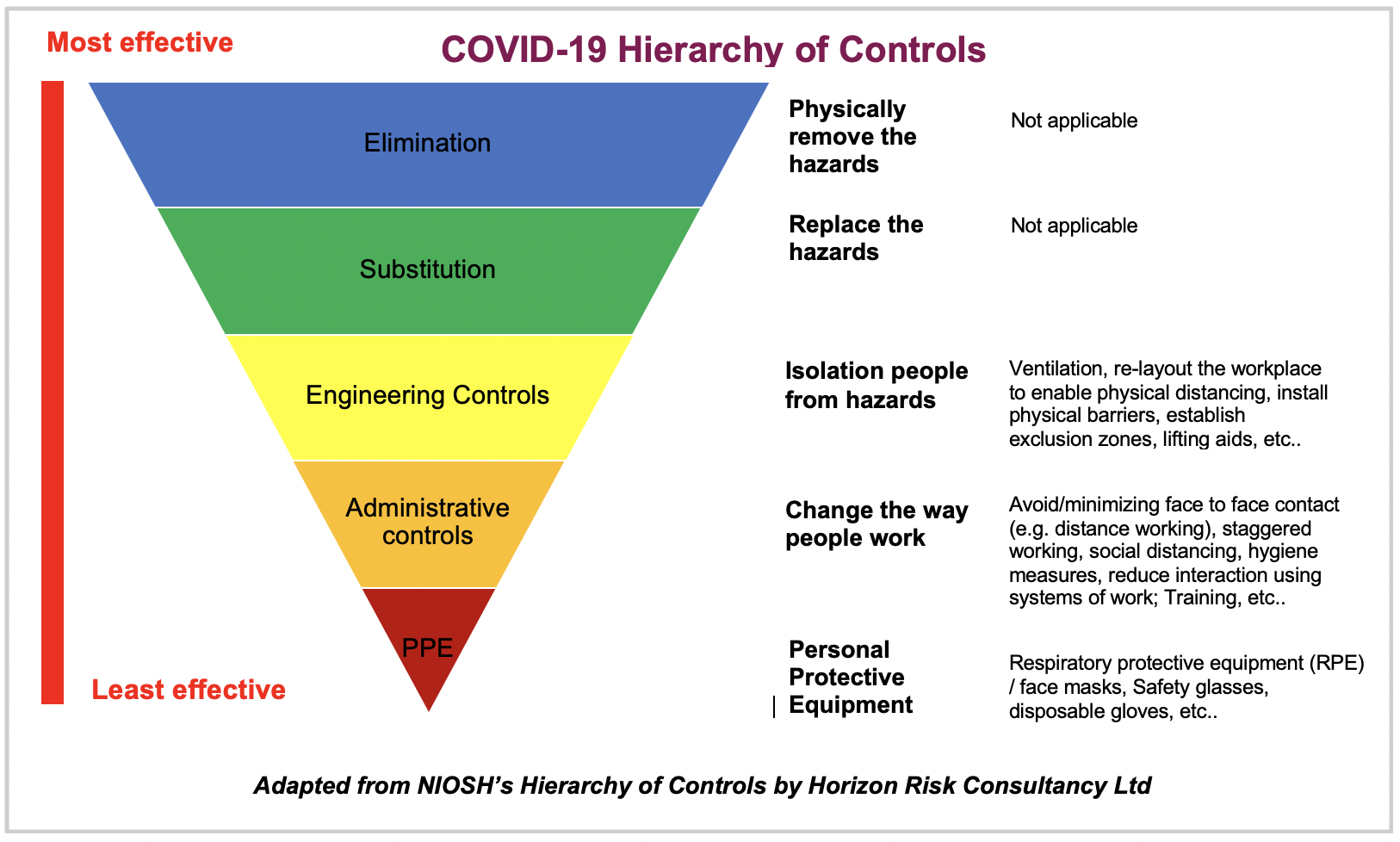
There are other models. One of the better ones for a workplace, or even for a country or economy, comes from the American Industrial Hygiene Association’s (AIHA) review of “hierarchy of controls” (HoC). Many union safety activists use this starter one from the National Institute of Occupational Safety and Health (NIOSH):

Note the engineering controls are elevated in effectiveness above PPE, in, for instance, preventing COVID infection and keeping the virus out of the workplace. It’s the presence of engineering and administrative controls such as testing, sick days, bringing in outside air, and filtering the air with upgraded filters that drive the greater part of infection outcomes in the workplace:
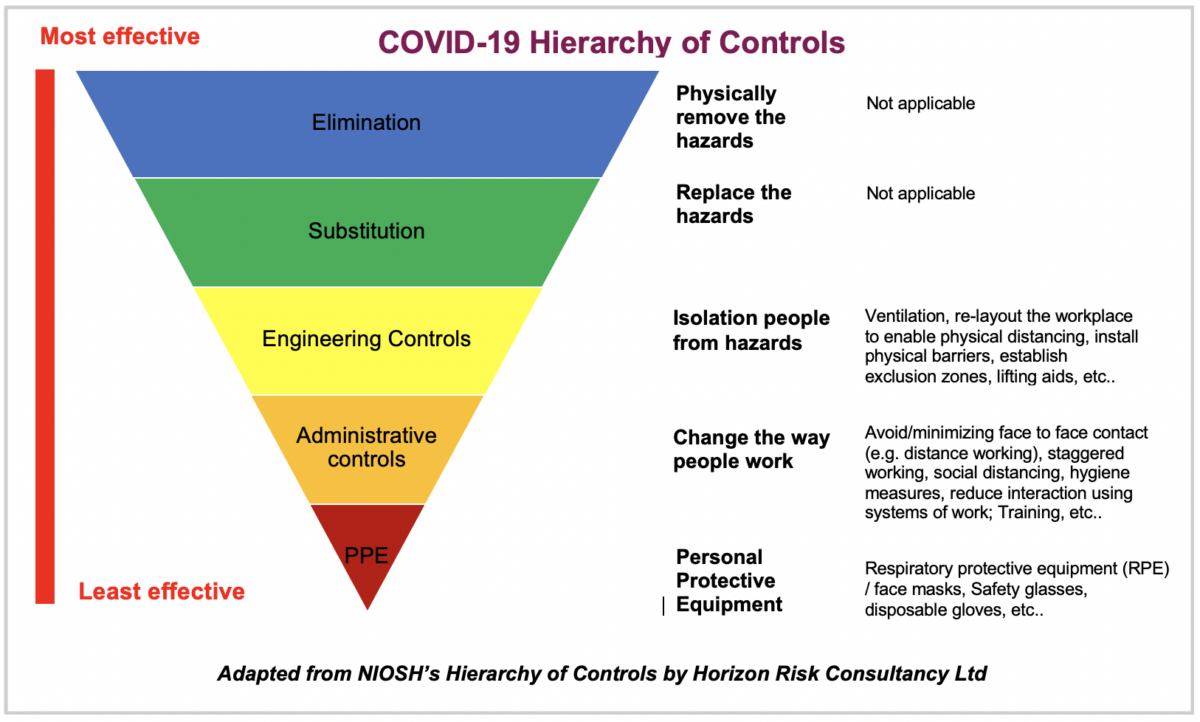
Horizon Risk Consultancy, the consultant that adapted the NIOSH HoC for COVID here, does not, however, recommend air filters, HVAC upgrades or paid sick leave.
{kind=link}
Here’s a more comprehensive version of the COVID HoC model from Doctors in Unite, the British medical union, including changes in ergonomics, working outside or from home and wage protections:
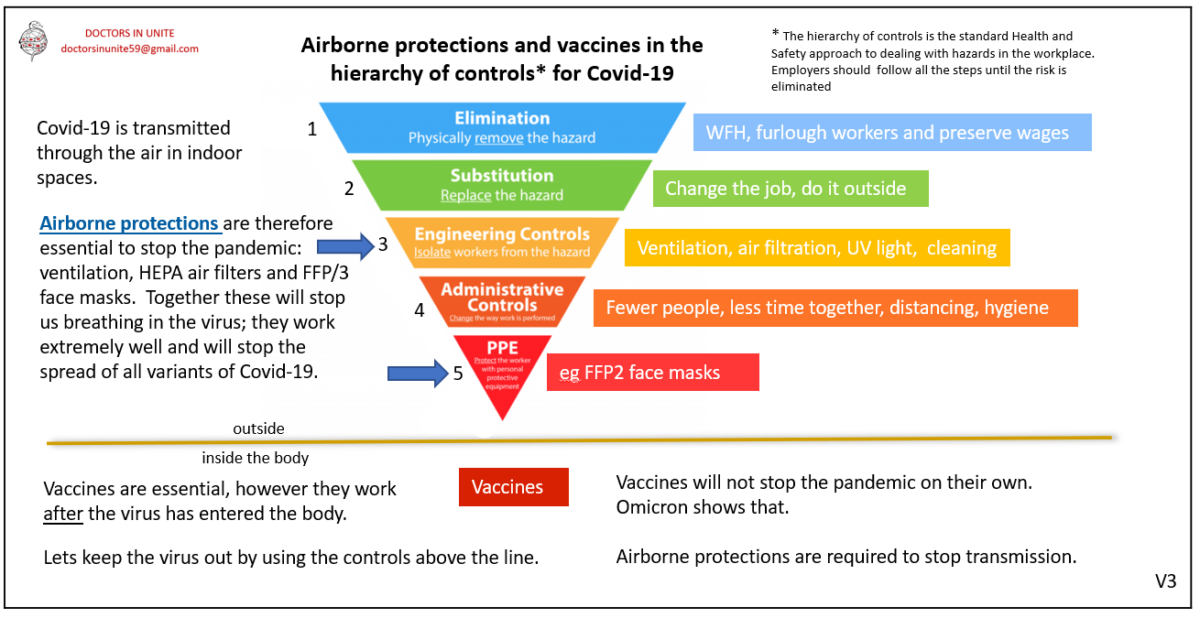
The full array of possible COVID-specific interventions inside the body and out are gathered in one graphic, including vaccination, face masks, distancing, ventilation, remote work, and, if necessary, furlough.
Public — Not Private — Prevention Must Be Our First Responder
We see the most effective occupational intervention is to keep the hazard outside the workplace.
Prevention through design — like building codes that design out fire risk — offers many professions, including building engineers, building inspectors and sanitation workers, opportunities to serve as public health heroes and save lives. In a prevention framework that extends beyond the individual, these are our true first responders.
The important work that firefighters, nurses, doctors and EMTs conduct should be embraced, of course, but also understood as the second and third lines of public defense. If a patient’s first encounter with a professional about their heart problem is a paramedic, society failed that patient.
Public health ecologists Deborah Wallace and Rodrick Wallace argue the modeling of emergencies, however necessary, often misses when and where the emergency begins. Structural causes — including expropriation, patriarchy and white supremacy — are as much part of the emergency, a bigger picture public health movements should assimilate in the face of the present administration’s efforts to censor such understanding.
This framework of prevention also puts engineers, architects, sheet metal workers and other trades in a position to design and construct buildings that inhibit the spread of airborne diseases. Preventing hospital visits saves both lives and money, but in ways that — contrary to the policies of Kennedy and Oz — place responsibility on those with the power to intervene at scale.
The entire design and construction professions, beyond essential public health measures like redesigning meat processing plants and following the new LEED certification that includes indoor air quality standards, should collaborate with unions in redesigning every workplace and all public spaces to better public health.
In other words, even the very best of the Swiss cheese models miss arguably the most critical interventions of all: the very package in which the slices come. While the diagrams show individuals, the government and even corporations, they do not show any organization of workers themselves — from unions to broader communities and how we choose to organize our society.
It is the responsibility of workers’ organizations, whether in the workplace or in the greater community, to push for the implementation of these safety protections — often of stunning epidemiological impact — in a society that presently denies them as a matter of principle.
Other parts of the bigger picture are still missing. Individual buildings and workplaces successfully eliminating COVID and future outbreaks will slow, but not end, pandemics.
Ultimately, preventing most zoonotic pathogens from emerging in the first place will better position us to bring the “age of pandemics” to an end. We can protect nature from the doomsday extractivism driving disease emergence by deploying regenerative agriculture, agroecology, conservation, regional planning, land back movements, and cooperative agro-economies. We can return the locus of control around what to grow to farmers and farming communities while also integrating Indigenous knowledge.
That is, we should better integrate collective choice and mutual economics up and down scales of social organization, across sectors and over our shared landscapes.
MAHA Public Health Is No Such Thing
Building on the back half of the Biden era, the Trump administration appears intent on exactly the opposite trajectory. It seems to be aiming to convince people that public health itself is the danger and removing it is a societal advance.
The resulting stops on the administration’s MAHA campaign trail have been shameless in their misdirection.
In April, RFK Jr. shared with tribes in Arizona and New Mexico the administration’s intention to prevent chronic disease in Native American populations. The administration, however, had just effectively ended the CDC Healthy Tribes program by mass firing program staff. The program deployed traditional medicine and foods to tackle disproportionate rates of chronic conditions, including diabetes and liver disease.
RFK Jr.’s announcement that HHS would prompt the food industry to remove synthetic dyes still left in the food system was juxtaposed with reports only a week earlier that the FDA would be ending federal-level food safety inspections and quality control programs for food testing laboratories.
The FDA had also just closed out an unpublicized investigation of a 15-state E. coli outbreak. The agency’s internal report on the outbreak didn’t even name the food suppliers and distributors involved, part of a broader abandonment in informing the public about outbreaks since the inauguration.
Oz’s swearing-in ended in a similar if more allegorical fashion:
Television personality Mehmet Oz was sworn in as the new administrator for the Centers for Medicare and Medicaid on Friday, but the Oval Office ceremony ended when a girl family member fainted.
A reporter was about to ask a question when the incident occurred, and Trump looked over at what was happening. White House staffers could then be heard shouting “press out” and “get out right now.”
With an empty gesture at a diagnosis:
Trump then went over to see what happened, and could be heard saying, “She’s OK.”
By that flippant assurance, found more widely in the MAHA program, a country is all well when it ends well. And by many a measure of what counts as a functioning society, the new administration signals its intent on wrapping up the project called the United States. A country without public health operating at scale can scarcely survive as such a thing — unless Americans organize together to get public health locked in as a central public tenet.
This piece was adapted from Pandemic Research for the People Dispatch #10 on collective choice and public health.
Media that fights fascism
Truthout is funded almost entirely by readers — that’s why we can speak truth to power and cut against the mainstream narrative. But independent journalists at Truthout face mounting political repression under Trump.
We rely on your support to survive McCarthyist censorship. Please make a tax-deductible one-time or monthly donation.