Honest, paywall-free news is rare. Please support our boldly independent journalism with a donation of any size.
On the campaign trail, President Joe Biden pledged to tackle the opioid crisis and remove federal restrictions on buprenorphine, a lifesaving treatment for opioid addiction. So far, the Biden administration has surprised doctors and addiction experts by moving in the opposite direction.
The Biden administration recently blocked an effort to expand access to buprenorphine, a drug the Biden campaign correctly called a “gold standard” for treating opioid addiction. Major medical associations and public health advocates who had applauded the effort, which came in the final days of the Trump administration, were left disappointed by Biden. On Wednesday, the White House said lifting restrictions on addiction medications remains a priority.
Fatal drug overdoses soared under President Trump and are now alarmingly high. The Trump administration was roundly criticized for blocking innovative efforts to prevent overdose and prioritizing the war on drugs over public health, and the reasoning behind the decisions made by both administrations remains murky. Both moves point to a growing conflict between policymakers, bureaucrats and law enforcement over prescription opioids that is blockading efforts to expand addiction treatment and, as emerging research suggests, may be contributing to a spike in fatal drug overdoses.
On January 7, Elinore McCance-Katz, the assistant secretary for mental health and substance abuse under President Trump, joined dozens of other officials in resigning after Trump motivated a violent mob to attack the Capitol. Reporting by The Washington Post suggests that McCance-Katz’s colleagues at the Department of Health and Humans Services (HHS) saw an opportunity in her early resignation and moved quickly to remove a major barrier to buprenorphine treatment during Trump’s last days in office.
McCance-Katz, who came under fire last year for echoing Trump’s talking points on COVID, resisted calls to suspend outdated rules requiring doctors to take a training course and apply for a special “X waiver” to prescribe buprenorphine. The X waiver rules, which limit the number of patients a doctor can treat with buprenorphine, are widely blamed for creating a nationwide shortage of doctors who are both willing and legally able to prescribe the drug. Methadone, another “gold standard” addiction treatment, is subject to even stricter regulation.
Barriers to a Life-Saving Treatment
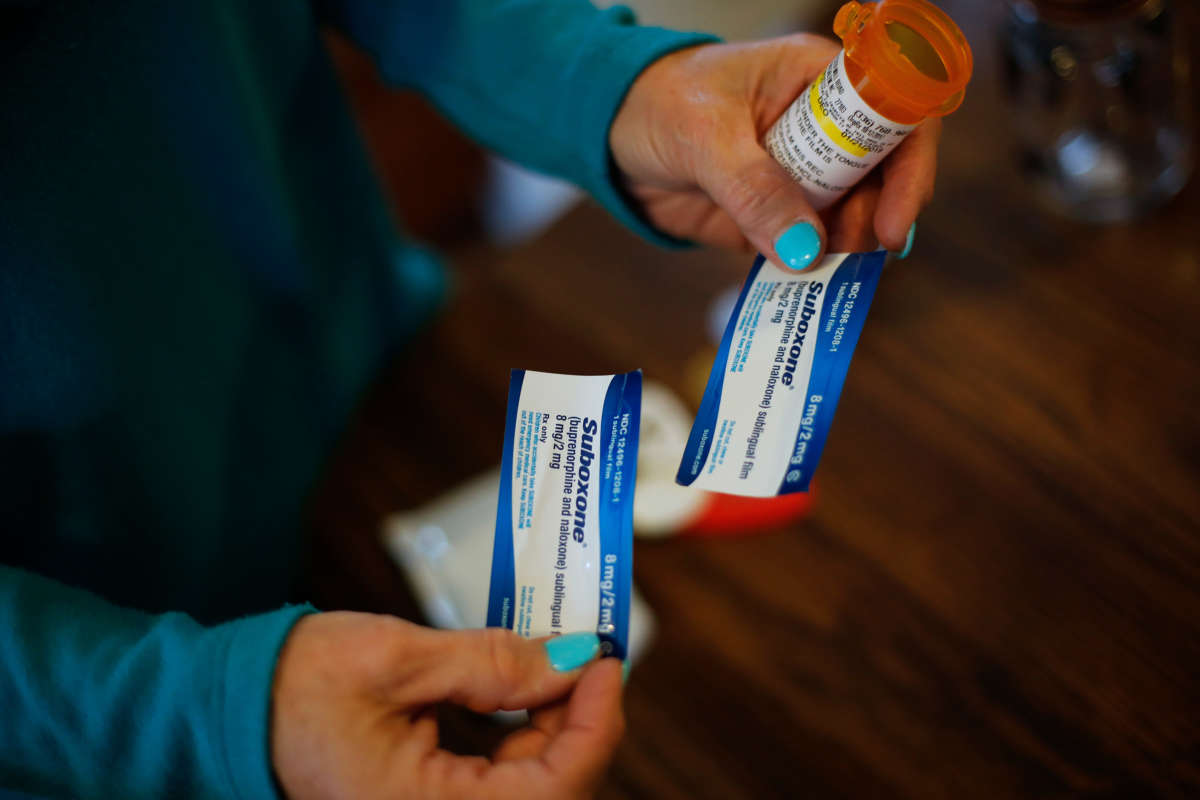
Like methadone, buprenorphine is an opioid that treats addiction by relieving painful withdrawal symptoms. The opioid antidote drug naloxone is included in leading buprenorphine formulas such as Suboxone, which does not cause the same euphoric effect as other opioids and is designed to prevent overdose. Still, buprenorphine is highly regulated compared to prescription painkillers. Along with law enforcement interventions that have a chilling effect on doctors and pharmacists, experts say the X waiver reinforces stigma that discourages doctors from becoming prescribers.
In France, where all medical doctors are allowed to prescribe buprenorphine without special licensing, opioid overdose deaths have fallen by 79 percent since 1995. Compare that to the United States, where only 5.7 percent of physicians have an X waiver to prescribe buprenorphine, leaving 39 percent of counties without a single prescriber, according to addiction advocacy group Shatterproof.
Doctors and pharmacists who prescribe and dispense buprenorphine are subject to Drug Enforcement Agency (DEA) inspections, and the drug war agency has raided and preemptively shut down addiction treatment clinics and specialty pharmacies while publicly conflating medical practitioners with drug cartels. Shatterproof reports that only 4.3 percent doctors publicly disclose that they can prescribe buprenorphine, and only a small portion prescribe to the maximum number of patients allowed under the X waiver. Doctors may be intimidated by law enforcement or suspicious of patients due to stigma around drug use that is reinforced by the X waiver.
Kevin Roy, Shatterproof’s chief of public policy, said the shortage of prescribers disproportionately impacts rural areas and communities of color that are chronically underserved by the medical system to begin with. He described treatment access as a “segregated system.”
“You’ve got a legitimate treatment that saves lives that people need, and if they can’t access it, their addiction is going to drive them to other alternatives,” Roy said in an interview.
After McCance-Katz’s resignation, the Post reports, HHS officials moved quickly to replace her with an acting assistant secretary who would allow a last-minute push to weaken the X waiver. HHS appeared to be trying to make up for lost time in the Trump administration’s final days.
Rates of fatal drug overdose increased during Trump’s time in office and ballooned after early 2019, with a record 81,000 deaths occurring over the 12-month period ending May 2020, according to federal data. While there are many factors and drugs besides opioids behind the increase in death, barriers to effective addiction treatment are certainly among them. The increase occurred despite billions of dollars in federal spending on the opioid crisis and a significant reduction in opioid prescribing. Trump boasted about fighting drug cartels, but nearly half of the estimated 2 million people living with opioid addiction in the U.S. did not receive treatment in 2018.
On January 14, HHS announced new guidelines that would allow doctors to prescribe buprenorphine without an X waiver if they are licensed by the DEA to prescribe controlled substances. Doctors and advocates said the changes did not go far enough — the new guidelines would have allowed doctors without a waiver to treat only 30 patients at a time, for example — but they applauded the move as an important first step.
A week after Biden’s inauguration, the Post reported that the Biden administration would not allow the guidelines to move forward. Doctors who treat addiction said the move was a “mistake.” In a statement, Biden’s HHS said the guidelines were “premature” and “cannot be issued at this time,” but the administration would “examine ways to increase access to buprenorphine, reduce overdose rates and save lives.” Anonymous sources at HHS told the Post that the hasty rulemaking had procedural problems within the federal bureaucracy.
In a statement on Wednesday, the White House listed “lifting burdensome restrictions” on medications for opioid addiction among its priorities for the first 100 days of Biden’s presidency. Advocates hope his administration will quickly issue a new set of buprenorphine guidelines on firmer legal footing. They are encouraged by Biden’s picks for top positions at the Office of National Drug Control Policy, including Deputy Director Regina LaBelle, and addiction expert who served in the Obama administration and has a background in public health rather than law enforcement. Biden has been laser-focused on the COVID pandemic, but advocates emphasize that public health crises do not exist in a vacuum.
However, Biden’s strategy for addressing the opioid crisis contains dangerous and punitive policies rooted in the failed war on drugs, such as arresting drug users and forcing them into mandatory treatment that can increase the risk of fatal overdose. The Biden administration may also face political pressure from the DEA and other law enforcement agencies, which have cracked down on prescription opioids in response to the overdose crisis – including buprenorphine and methadone, which are proven to prevent overdose.
Advocates and medical associations are also looking to Congress, where bipartisan bills to repeal the X waiver have been introduced two decades after lawmakers originally created the notorious barrier to treatment.
“We’re certainly disappointed that the guidelines weren’t enacted, but there is a bigger policy issue at hand, and that is ensuring the law is changed so that all prescribers — not just physicians — can provide ready access to this treatment,” Roy said. “Congress shares a vital role in this.”
The Supply Reduction Fallacy
The government’s response to the opioid crisis is a dangerous blame game. Journalists and officials have pointed fingers at drug manufacturers and then the DEA, which were accused of working too closely with each other and failing to control the pharmaceutical opioid supply for over a decade. The U.S. has always suffered a shortage of addiction treatment providers, but narratives around opioid overprescribing dominated the conversation for years as the media told sensational stories about celebrities and suburban teenagers moving from painkillers to street drugs.
While the effort began under President Obama, the Trump administration and a number of lawmakers took on the mission of reducing the supply of opioid painkillers with vigor. New restrictions were put on painkiller prescribing, and states set up digital databases allowing law enforcement to monitor patients, doctors, pharmacists and prescriptions. The Trump administration funneled billions of dollars from Congress toward increasing access to addiction treatment, but the X waiver remained.
As the DEA raided clinics and pharmacies, doctors began forcing patients with chronic pain to taper off or even stop opioid treatment, and pharmacists became increasingly wary of dispensing buprenorphine, according to interviews with pharmacists and patients. The DEA now accuses pharmacists of fueling the opioid crisis by filling legitimate prescriptions written by physicians. Some chronic pain patients filed lawsuits against major pharmacies for refusing to fill prescriptions; others committed suicide or began buying dangerous alternatives illegally, increasing the risk of overdose.
A recent case-control study of patients who received opioids for chronic pain in Colorado found that patients who later used heroin were roughly twice as likely to have had their opioid prescription cut off by their doctors. In Canada, a 2020 study found a correlation between reductions in opioid prescribing and increases in overdose deaths, with the two provinces where prescribing dropped the most recording the largest increases in opioid-related deaths. The authors concluded that fewer pharmaceutical pills available on the street lead to more “non-medical opioid users” turning to heroin and fentanyl.
The DEA now boasts that the number of prescription painkillers on the legal market has dropped to its lowest point since 2006. Rates of fatal overdose from prescription opioids dropped as well, but overdose deaths involving heroin and fentanyl are skyrocketing. While overdose deaths involving stimulants have also increased during the COVID pandemic, deaths involving fentanyl increased 38 percent during the 12 months leading up to May 2020.
At the heart of the failed “supply reduction” approach is law enforcement’s obsession with “diversion,” the idea that people obtain opioid prescriptions to sell the drugs. McCance-Katz and other opponents of lifting the X waiver, as well as prison wardens who refuse to provide vital addiction treatment to incarcerated people, cite overprescribing and “diversion” of buprenorphine as a top concern. This thinking is rooted in the failed war on drugs, which criminalizes vulnerable people and has thwarted public health efforts for decades.
In fact, Roy and other experts agree that the buprenorphine-naloxone formula is safer (and far less pleasurable for non-patients) than prescription painkillers. Multiple studies along with plenty of anecdotal evidence suggests that buprenorphine is primarily “diverted” to people who live with untreated opioid addiction and wish to avoid withdrawal, making them candidates for buprenorphine treatment in the first place.
Patients at Risk of Relapse Without Access
Tessa is a public health worker in the U.S., and she knew she needed a prescription for the buprenorphine formula Suboxone. Tessa, whose full name has been omitted to protect her privacy, successfully used Suboxone for three years during her recovery from heroin addiction. She decided to taper off when moving to a different state in 2019 because obtaining a new prescription would be difficult. About a year later, as the COVID pandemic added to life’s daily stresses, Tessa was on the verge of a relapse.
After calling her insurance company and being directed and redirected through a series hotlines and potential providers, Tessa learned that it could take up to two and a half weeks, along with showing up for a series of appointments and medical tests while working a full-time job, to finally see a doctor who could prescribe Suboxone. Meanwhile, it took five minutes to find heroin on Craigslist.
While Tessa did access Suboxone and maintain her recovery, she remains frustrated by policymakers who refuse to lift the X waiver.
“I think the reality of it, coming from my personal experience, is feeling incredibly desperate and afraid,” Tessa told Truthout. “It’s scary to think that something that has been really beneficial and helpful for my recovery could be taken away or really difficult to access.”
She emphasized the disparities in access to buprenorphine.
“We are making it really difficult to access, especially for people who are unhoused or people who have more economic insecurity,” Tessa added.
Like others in the world of public health and harm reduction, Tessa envisions making buprenorphine available at clinics and harm reduction sites where drug users already access safety supplies, such as clean syringes and naloxone, to prevent overdose. Addiction treatment, Tessa says, should be available on-demand to people who are ready to begin treatment, not hidden behind federal regulations and suspicious insurance providers.
Whether Biden will listen to drug warriors or to doctors and real-life experts like Tessa remains to be seen, but the fate of the X waiver will signal which direction the new administration is heading.
Fundraiser Deadline: Missed
Truthout is one of only a few platforms for justice-oriented, grassroots journalism. Today, as political censorship from the right intensifies, we have no choice but to ask for your help.
We missed our fundraising deadline, but there’s still time to help us meet our basic operating expenses before the end of the month. If you can support Truthout with a one-time or monthly donation, you will make a significant impact on our work. Anything you can do makes a difference — we appreciate your support.