Truthout is a vital news source and a living history of political struggle. If you think our work is valuable, support us with a donation of any size.
Indulge me. Imagine you take a medication that is vital to your health: as vital as oxygen or water. You can’t go a single day without it because you are completely dependent on it to think, to work, to take care of your family, to just be you. And if you miss a dose? A withdrawal hellscape awaits: extreme muscle and bone pain, intense cravings, vomiting, insomnia, severe anxiety, cramps, cold sweats, fever, and bouts of diarrhea. Death might actually be preferable. What kinds of indignities would you endure to avoid that experience? How far would you go to get the drug that literally saves your life every day?
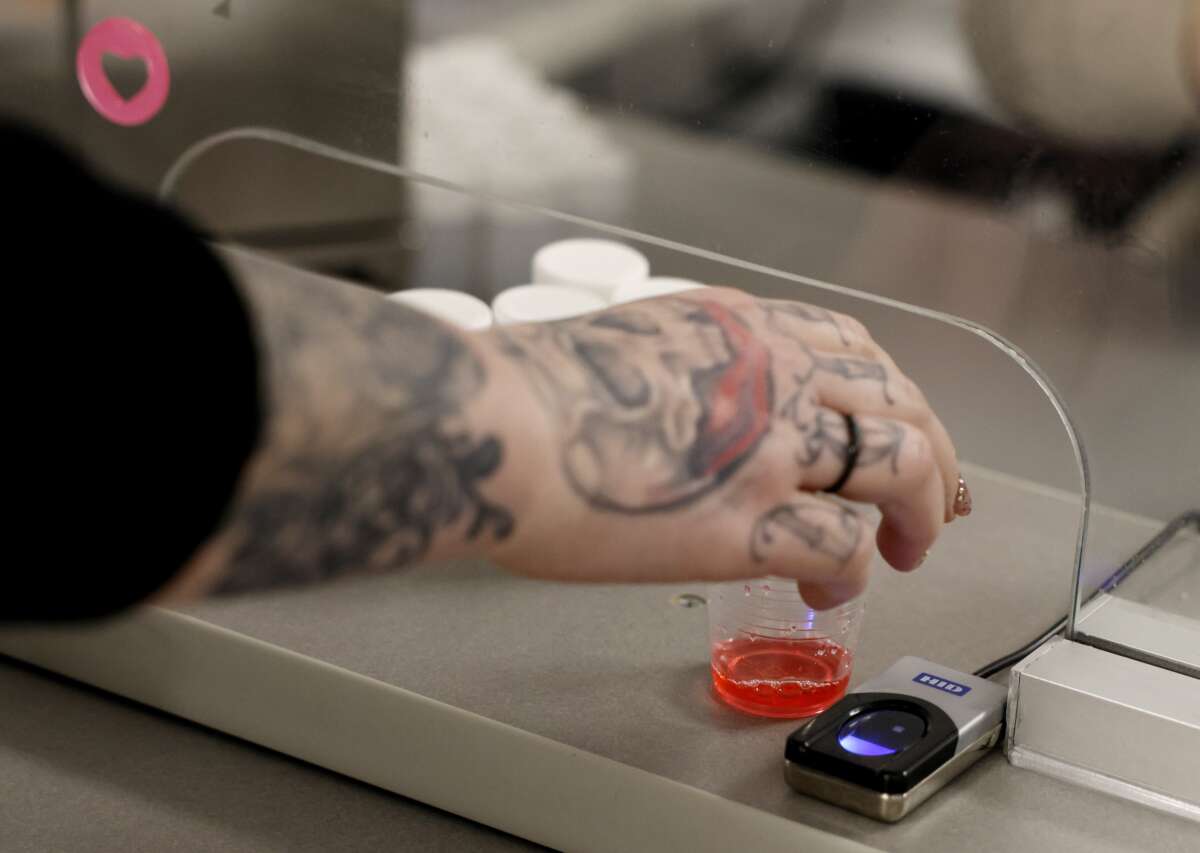
Be honest: You would do whatever it takes to get it — and it, in this case, is methadone. And the only way to legally obtain this medication that mercifully binds to mu-opioid receptors and blocks the brain from telling the body to revolt is to attend a special clinic six or seven days a week and be observed by a nurse swallowing the medication. These methadone clinics, also known as opioid treatment programs (OTPs), are licensed and regulated through a partnership between the Drug Enforcement Administration (DEA) and the Substance Abuse and Mental Health Services Administration (SAMHSA). That the DEA, a police organization that is waging the War on Drugs, is involved in the dispensing of methadone is outrageous. They are ignorant about the nature of addiction and believe that methadone is a dangerous drug and that adults who take it cannot be trusted. That SAMHSA, an agency composed of medical doctors, addiction experts, and researchers who do understand the importance of methadone to treat addiction, collaborates with DEA drug warriors is also outrageous. Their decades long partnership has denied people who need methadone their freedom.
Methadone is a full agonist, synthetic opioid used to treat addiction to heroin, fentanyl, and prescription opioids like oxycontin. It eliminates intense cravings and withdrawal. The medication is the gold standard of treatment. It was discovered by doctors Vincent Dole, Marie Nyswander, and Mary Jeanne Kreek at Rockefeller University in the 1960s. A report by the National Academy of Sciences Institute of Medicine (IoM) concluded, “Methadone maintenance has been the most rigorously studied drug treatment modality and has yielded the most incontrovertibly positive results…. Consumption of all illicit drugs, especially heroin, declines. Crime is reduced, fewer individuals become HIV positive, and individual functioning is improved.”
The IoM also noted that methadone can be taken as a maintenance medication with few negative side effects. In reviewing clinic regulations, though, the researchers also concluded, “Current policy puts too much emphasis on protecting society from methadone, and not enough on protecting society from the epidemics of addiction, violence, and infectious diseases that methadone can help reduce.” The report was published in 1995.
Tragically, society is still being protected from methadone. That’s because the drug has been locked inside a singularly oppressive penal institution that is anchored in a culture of cruelty and surveillance. The DEA, SAMHSA, and OTPs have created dense layers of nonsensical arbitrary rules and regulations that make entering and staying in a program a frustrating and humiliating daily ordeal. In the midst of an ongoing overdose crisis, just one in five adults received medication to treat opioid addiction, with women and African Americans substantially less likely to have access. Longer retention in methadone treatment is associated with better patient outcomes, and research indicates the first twelve months are critical to patient success. Studies over decades show that the majority of patients drop out during the first year of methadone treatment, with one study showing that 64 percent of patients discontinue use of medication prior to six months.
Yet drug warriors and callous bureaucrats in these federal agencies, along with clinic staff, shift the blame to patients. They don’t “follow the rules,” they don’t “take recovery seriously,” or — the biggest lie of all — patients are “not ready for treatment.” Patients don’t fail methadone treatment; the treatment fails them. Methadone itself is a tool of harm reduction. But the clinics that control methadone are a system of harm production that drives people out of treatment and back to a toxic supply of street drugs. Over one million Americans have died from opioid-related overdoses. Methadone has been proven to cut the overdose death rate by 59 percent. It is criminal that OTPs take a medication with such demonstrated, lifesaving benefits and make it difficult to access.
Carceral Clinics
Imagine you’ve just stepped off a crowded bus after a second subway transfer, or you’ve just driven a white knuckled harrowing hour during a snowstorm, and you pull up to an unmarked concrete building with frosted windows that is surrounded by a tall black steel fence in the “seedy part of town.” It’s 5 a.m. There is a line of people snaking around the block. You join it. This is where you come to swallow one dose of liquid methadone six or seven days a week.
Every interaction between patients and staff in the methadone clinic system is marked by a lack of trust, surveillance, coercion, and punishment. Patients are not allowed to possess their own medication. Instead, a constantly changing cast of counselors, security guards, physicians, and nurses control access, robbing patients of autonomy while exerting control over their lives well beyond the walls of the OTP.
This massive power imbalance, which is rarely acknowledged, creates an environment that keeps patients passive, afraid, anxious, and obedient. In no other health care setting are patients with chronic medical conditions at the complete mercy of staff and constantly threatened with being cut off their medication and forced into withdrawal. This practice is a human rights violation and contravenes the Hippocratic Oath and the Nursing Code of Ethics, which declare “do no harm” and promote “autonomy in decision-making and justice.”
Commuting to a clinic is a lifelong proposition. A counselor said to Louis Jones, a former methadone patient in New York City, “Till death do we part.” Patients routinely talk about OTPs using carceral language. They are on chemical parole or a chemical tether, restrained by liquid handcuffs; attending the clinics constitutes a life sentence; the clinic is a ball and chain; patients are lifers. Indeed, the relationship between staff and patients models a prisoner-guard relationship. The clinic assigns everyone an ID number, and some nurses use that instead of the name of a person to confirm their identity and dose.
I had no idea what I was getting into. In the beginning, it didn’t bother me having to go to the clinic six days a week because it gave me a reason to wake up every morning. But after a year passed, I realized it was a prison because I couldn’t go anywhere without having this drug with me, and I couldn’t get take-home bottles. I don’t care if I was going to the clinic once a month or once a week, it was still a prison.
–Francine, New York
The resemblance to prisons is a feature, not a bug, of the clinic system. Methadone clinics were designed to segregate, control, and monitor patients, much like penal institutions. When a person enters a clinic, they lose their freedom and basic human rights. Uniformed security guards are the first personnel patients encounter. Some clinics hire off-duty cops. The job description for a security officer at Montefiore OTPs in the Bronx includes managing the waiting area and directing patients to medicating windows; exercising constant vigilance of patients, staff, and visitors; and performing perimeter patrols, including loitering patrols. The job qualification section states “military experience preferred.”
Loitering or “hanging around” the vicinity of clinics is taken very seriously. This is because the neighborhoods OTPs are located in have opposed their opening and are looking for reasons to shut them down. When the Greater Harlem Coalition complained about loitering at a Mount Sinai OTP in Harlem, the management agreed to “contract a new, more reputable security firm and staff their new building with retired New York Police Department (NYPD) sergeants and install additional security measures inside the buildings, such as metal detectors and security cameras.”
A sign posted on the door and in windows of the Family Guidance Center in Chicago threatened: “If you are seen loitering or lingering around the building or the surrounding area, you will immediately be placed on involuntary withdrawal.” The sign speaks volumes about the oppression of people who take methadone. That a health care facility would force a patient into withdrawal for simply lingering in the vicinity of the clinic is barbaric.
Policing patients is a core function of clinic security guards, and police officers in the community have harassed and arrested patients on their way to the program and while waiting in line outside. The Beyond Methadone study in New York City found that nearly four in ten patients surveyed reported being stopped and frisked by police outside their clinic, and seven in ten respondents witnessed someone else being frisked or harassed by police while entering or leaving the clinic. A methadone patient explained, “The police arrested a few of the people on the program…. If they need a spot to meet their quotas, they just come to the methadone programs and mess with people, search them for no reason…. I have missed a dose because of the police.”
At a New York City clinic I filmed in for my first documentary, a guard sat in a raised booth in front of the entrance to the medicating area. As patients arrived, he ordered them to throw take-out coffees, plastic water bottles, and cans of soda into a large trash bin. This was a security measure to prevent diversion of methadone. Inside the booth, a bank of monitors displayed camera feeds from all areas of the clinic and tracked the movement of people inside and outside the building. This is how patients are caught loitering or breaking other clinic rules. Doug was in line waiting for the clinic to open and got into a brief pushing match with another patient who cut the line. No one was hurt, but later staff confronted him with the footage of the altercation and kicked him out of the clinic permanently for fighting.
Security officers are stationed in OTPs for another critical reason. At the American Association for the Treatment of Opioid Dependence (AATOD) conference I attended in 2022, Dr. Kenneth B. Stoller, the director of Johns Hopkins Broadway Center for Addiction in Baltimore, stated, “Security is there to make staff feel safe.” But safe from whom? The pervasive presence of uniformed security personnel and hyper-surveillance in clinics creates an atmosphere of criminality and hostility while reinforcing the power imbalance.
Many clinics operate in old run-down buildings with unmarked facades surrounded by razor wire-topped fences in abandoned, deindustrialized zones full of detritus to deter NIMBY protests. A clinic in East Harlem has separate entrances for patients and staff. Iron bars on windows and roll-down metal security gates are common. Clinic interiors are austere and cold, with artificial lighting, drab colors, and ceiling mounted cameras. Methadone clinics have long embodied hostile architecture before it became a thing on Instagram. There is no art, beauty, or comfort in clinics because of their prison-like environment.
In dense urban areas like New York City, OTPs hide in plain sight with no signage and tinted windows. An unmarked storefront clinic on the Lower East Side has graffiti sprayed across it and the glass is blacked out. In 1971 a methadone program that was closed by the DEA transferred all their patients to the Gold Star Mother, a decommissioned Staten Island ferryboat that was docked at Battery Park on the Hudson River. “Every weekday, 450 former heroin addicts climb a gangway to the Gold Star Mother. . . . After showing their credentials and submitting to tests, they climb to the upper deck. At what used to be the refreshment stand (the soft drink machines have not yet been removed) they receive one-day dosages of methadone.” Two OTPs in Boston located on “Methadone Mile” are around the corner from the Suffolk County House of Corrections. A coincidence? In rural Pennsylvania, an OTP is housed in a cross between a shipping container and a trailer. A concrete building with no windows in Baltimore accommodated a storefront church, the New Life Evangelical Baptist Church, and a methadone clinic.
OTPs are purposely invisible. They’re not businesses the public is supposed to see or be able to identify. The only thing that gives them away is the people standing in long lines outside the building. Imagine having to spend any amount of time inside or even outside such a dismal and depressing place for years on end.
Media that fights fascism
Truthout is funded almost entirely by readers — that’s why we can speak truth to power and cut against the mainstream narrative. But independent journalists at Truthout face mounting political repression under Trump.
We rely on your support to survive McCarthyist censorship. Please make a tax-deductible one-time or monthly donation.